
Evolution of US Payer Management of Oncology, an examination of Non-small Cell Lung Cancer (NSCLC) and Chronic Lymphocytic Leukemia (CLL)
Evolution of US Payer Management of Oncology, an examination of Non-small Cell Lung Cancer (NSCLC) and Chronic Lymphocytic Leukemia (CLL)
By Two Labs‘ Anne Runyan, Daniele Severi-Bruni, Joe Honcz, and Mason Daniels. Two Labs is an industry-leading pharma services company based in Columbus, Ohio.
Background and Introduction:
It is well known that the cost of oncology drugs in the US is high and rising. In fact, US spending on oncology drugs increased 64% from $23.7 billion to $56.7 billion between 2015 and 2018 alone[i]. Despite the large increase in cost, US payers have historically not actively managed oncology drugs. Research conducted in 2017 confirmed that payers were primarily managing oncology drugs with traditional clinical management tools, such as prior authorizations, step edits, and quantity limits, which were mostly ineffective at managing cost[ii].
Methodology:
In order to better understand how US payer management of oncology has evolved in the past three years, we conducted an online survey with 25 Pharmacy Directors and Medical Directors at US insurance companies. The survey also monitored whether there were differences in management when looking at different indications within oncology. The individuals surveyed represented a total of 112.5 million covered lives. We also developed a formulary tracker which analyzes Pharmacy Benefit Manager (PBM) exclusion lists for 2021, to better understand whether payers are beginning to actively manage any categories within oncology. Finally, we conducted an in-depth discussion with a former P&T decision maker with experience at multiple national managed care organizations.
Topline Findings:
While payers are not actively increasing management in oncology as a whole, each oncology indication appears to be considered separately. We are starting to see a growing variability in the level of management across different oncology therapeutic areas. There are several characteristics to consider when determining if an indication within oncology may be managed by payers: size of the patient population, acuity/severity of disease, the availability of clinical trial data that can be used to directly compare agents, and the level of competition.
Payers are less concerned with managing indications with smaller patient populations, because the overall budget impact of these indications still remains manageable and usually there is not enough competition to allow differential management of therapeutically comparable agents. For indications with a higher mortality rate, payers are hesitant to restrict physician choice in any way. It is more challenging for payers to manage indications where there is a lack of comparable evidence across products. The emerging opportunity for a more rigorous management is in disease states that has are becoming more crowded with competitors, with highly comparable clinical evidence and with a disease state that is less aggressive. It is in these areas that some payers demonstrating a willingness and ability to manage.
Findings by Disease Area:
Chronic Lymphocytic Leukemia (CLL)
It is estimated that in 2021, 21,040 individuals in the US will be diagnosed with CLL. On average, patients are diagnosed at age 70. Despite an oncology indication, this disease has a favorable prognosis with a five-year survival rate of 85%.[iii]
In recent years, Bruton Tyrosine Kinase (BTK)-inhibitors have shifted the standard of care in CLL[iv]. There are currently three BTK-inhibitors on the market: Brukinsa, Calquence, and Imbruvica. A fourth product, Venclexta, is also indicated to treat CLL and has comparable data to the BTK-inhibitors. These drugs come with a high price tag, with WAC/year ranging from $157,497 to $181,669 and a three-year cost of up to $545,007.
Due to the high cost and the possibility for a long treatment duration, payers in our sample rated the overall budget impact of BTK-inhibitors as high (figure 1)

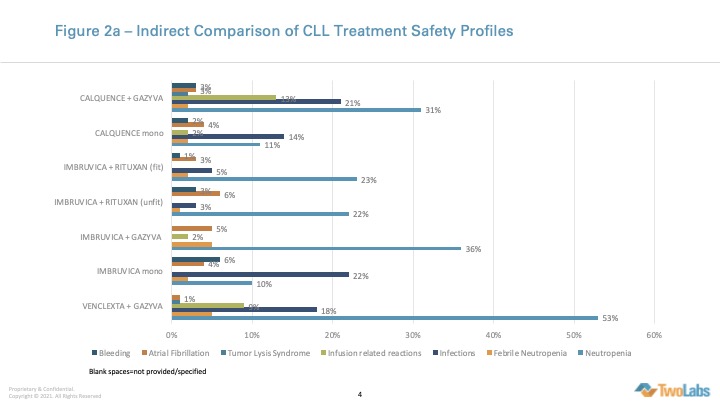
Due to the way clinical trials were designed, it is possible to make indirect comparisons of the safety and efficacy of each CLL agent. The resulting analysis has noted that there is minimal differentiation across products (figures 2).

When payers were asked to rate the therapeutic value of each BTK-inhibitor on a scale of 1 to 5 where 1 is no therapeutic value and 5 is a breakthrough therapeutic innovation, they gave similar scores for each agent (figure 3)

None of the payers in our sample were currently managing any BTK-inhibitor beyond NCCN guidelines in 2020. In three to five years, four payers expected that they would manage at least one BTK-inhibitor more restrictively than product label and placement in NCCN guidelines.
However, when the PBM exclusion tracker was analyzed, we found that Express Scripts (ESI), a PBM with influence over >60 million lives, listed Imbruvica and Venclexta as preferred options and excluded Calquence from formulary[v].
Discussions with a former payer suggest that if ESI has taken this action, other PBMs and Managed Care Organizations are likely to follow suit. He notes that “Nobody wants to be the first to take action, but once somebody else does, others will be fast followers.” He compares this to other disease categories which were historically “no touch” such as HIV. As the treatment for HIV moved from multi-tablet regimens (MTR) to single-tablet regimens (STR) payer began to slowly introduce utilization management (UM) tools such as prior authorization and step therapy. The frequency of UM tool increased in direct relation to the increasing number of STR approved. At this time most payers have followed suit and the category is now more managed than it has been in the last 20 years. He notes that there were also similar tipping points in anti-infectives and that it is a trend we are also now witnessing with an increased number of biosimilars.
Non Small Cell Lung Cancer (NSCLC)
NSCLC is the most common form of lung cancer, comprising 84% of all lung cancer diagnoses. The prognosis for NSCLC patients is poor with NSCLC making up 25% of all cancer deaths and a low five-year survival rate of 25%[vi].
Immune checkpoint inhibitors, such as PD-1 and PD-L1 inhibitors Keytruda, Opdivo and Tecentriq, have greatly improved the standard of care in NSCLC[vii].
Compared to CLL, payers in our sample rate the budget impact of PD-1 and PD-L1 inhibitors as moderate, and lower than CLL, however they expect this to increase in the future (figure 4).

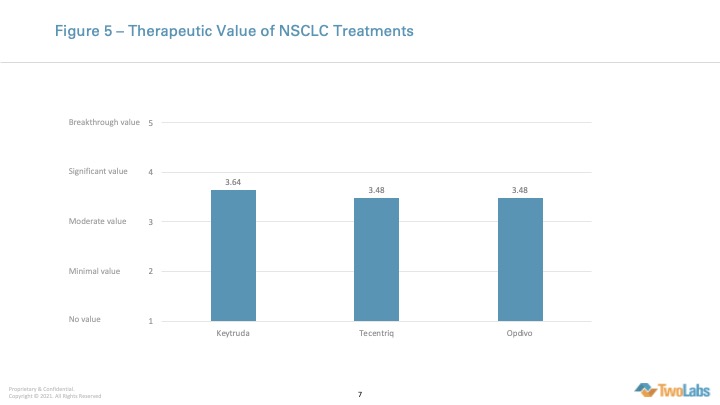
As with CLL, payers see minimal differentiation between products and rate all of the PD-1/PD-L1 inhibitors as having moderate to high clinical value (figure 5). However, we understand from a review of the literature that in NSCLC it is difficult to directly compare products, due to the way clinical trials are designed[viii].
Today, all but one payer in our sample indicates that they are managing PD-1/PD-L1 inhibitors to NCCN guidelines. Although five payers expect to manage these agents more restrictively in three to five years, this may be difficult to do in reality.
Review of the PBM exclusion tracker as well as MCO formularies confirms that PD-1/PD-L1 inhibitors are not restricted beyond label or NCCN guidelines. Discussions with a former payer suggest that the only restriction payers are currently using in NSCLC is to restrict site of care for expensive agents such as Keytruda.
Conclusions:
There are several reasons why BTK-inhibitors make a good category for payers to begin exerting control. The relatively high budget impact makes management a priority. The availability of data across products makes it possible to indirectly compare these agents and choose preferred and non-preferred options while leaving physicians with efficacious treatment options. Payers have some level of comfort managing CLL because of the acuity level. The disease has a lower mortality rate than other cancers and there is more time to treat patients, and therefore more time to try different agents.
Payers in our study rate the budget impact of NSCLC treatments as lower than that of CLL agents. The way that clinical trials are designed makes it difficult to compare products, which creates hesitation in management for payers. The high morbidity rate leaves little room for mistakes and as a result, payers are hesitant to limit physician choice. However, payers in our sample expect the budget impact of PD-1 and PD-L1 inhibitors to increase in the future. As budget impact increases, the data becomes more mature, the category becomes more crowded, and payers begin to feel more comfortable managing indications within oncology, NSCLC will be an important indication to monitor.
Overall, when thinking about the future of payer management of oncology drugs in the US, it will be useful not to think of oncology as a whole, but as a series of disease states, each with unique characteristics and considerations.
——————————————————————————————————————————————
[i] IQVIA, Global Oncology Trends 2019, Therapeutics, Clinical Development and Health System Implications, Institute Report, May 2019
[ii] Runyan A, Banks J, Bruni DS. Current and Future Oncology Management in the United States. J Manag Care Spec Pharm. 2019;25(2):272-281. doi:10.18553/jmcp.2019.25.2.27
[iii] Leukemia – Chronic Lymphocytic – CLL – Statistics. Cancer.net. Published June 25, 2012. Updated January 2021. Accessed April 21, 2021. https://www.cancer.net/cancer-types/leukemia-chronic-lymphocytic-cll/statistics
[iv] Cote B. Research efforts abound as the role of BTK inhibitors continues to evolve in CLL. Onclive.com. Accessed April 21, 2021. https://www.onclive.com/view/research-efforts-abound-as-the-role-of-btk-inhibitors-continues-to-evolve-in-cll
[v] Internal Two Labs Formulary Tracker Database
[vi] Lung cancer – non-small cell – statistics. Cancer.net. Published June 25, 2012. Updated January 2021. Accessed April 21, 2021. https://www.cancer.net/cancer-types/lung-cancer-non-small-cell/statistics
[vii] Yoneda K, Imanishi N, Ichiki Y, Tanaka F. Immune checkpoint inhibitors (ICIs) in non-small cell lung cancer (NSCLC). J UOEH. 2018;40(2):173-189.
[viii] Fessas P, Lee H, Ikemizu S, Janowitz T. A molecular and preclinical comparison of the PD-1-targeted T-cell checkpoint inhibitors nivolumab and pembrolizumab. Semin Oncol. 2017;44(2):136-140. doi:10.1053/j.seminoncol.2017.06.002
